

Health Advisory & Recovery Team | COVID-19 Weekly Bulletin
HART vs SAGE
HART Pathology Lead Dr John Lee appeared on Good Morning Britain this week alongside Professor Susan Michie who sits on SAGE and the Scientific Pandemic Insights Group on Behaviours (SPI-B).
Dr Lee noted the lack of evidence for asymptomatic spread of SARS-CoV-2 and also pointed out the absence of diverse scientific discussion in the media. Susanna Reid denied this, stating that the other side was being heard on social media and in the papers. However, these avenues are not the same as trusted mainstream TV programmes and the void of diverse thinking here has no doubt hampered the public’s understanding of ‘the science’.
Reid went on to say that ‘we know from the evidence that lockdown does work’. This is simply not true. Increasingly, the body of evidence points to the exact opposite as can be seen here and in dozens of published peer-reviewed papers, in stark contrast to the absence of evidence demonstrating significant benefits from lockdown when examining the real-world (as opposed to modelled) evidence. In addition, these models neglect to adequately assess the collateral harms.
Reid highlighted the figure of 126,000 COVID-19 deaths. However, there is a serious issue with excess, mainly non-Covid deaths at home which have reached over 50,000 in total. Here in the UK this figure currently sits at roughly 1,000 people each week. Perhaps many of these people would not have been put off seeking medical treatment had Michie, and her behavioural science colleagues, not terrified them into ‘staying at home’. A review of these covert, ethically questionable, psychological strategies was recently published by a member of HART here.
Michie also talked about mutant variants and how many people it is or is not ‘safe’ to interact with. It is a shame that these questions were addressed to a psychologist, rather than to a pathologist with medical training. No mention was made of the inevitable seasonal decline of the virus and Michie mentioned several thousand new cases a day, neglecting to outline how these figures relate to hospital statistics (currently at September levels).
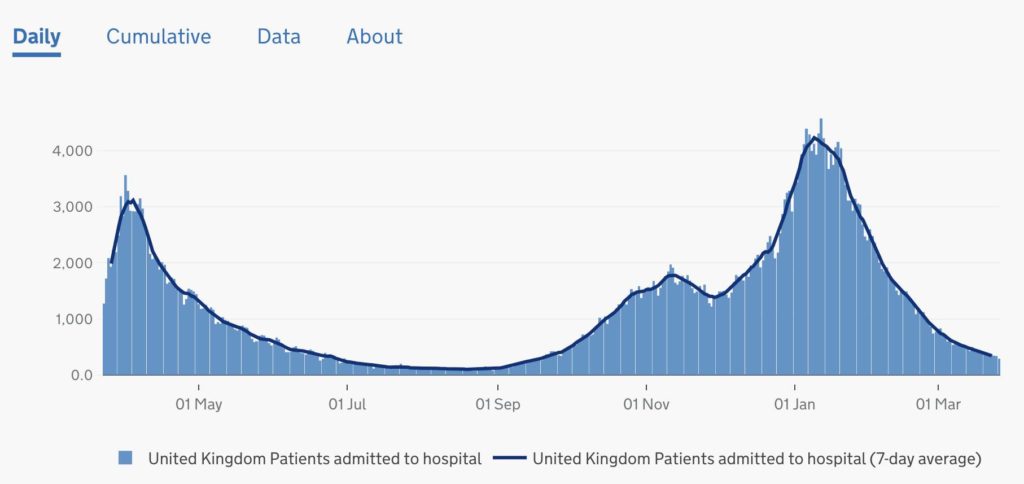
Patients admitted to hospital in the UK
In fact, we know from numerous studies that there will be a significant number of post infectious positives at this stage with patients admitted to hospital for other reasons, incidentally testing positive. In the community, the expected surge in cases in the secondary school population has not materialised and the results of testing show that there is no active SARS-CoV-2 in that population. Overall, there is minimal evidence of residual coronavirus in the community. Mitchie went on to say cases are rising in Scotland. Again, this simply is not true.
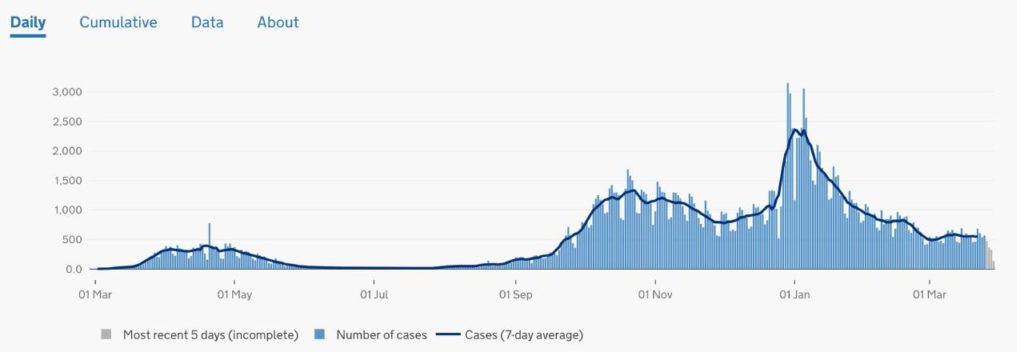
Cases in Scotland
Michie then described the possibility of exponential growth if we remove measures too quickly, which shows a misunderstanding of the current immunity status of the population. With so many now having antibodies through natural infection or vaccination, it seems highly unlikely that this virus could now spread in an epidemic fashion. A transition into an endemic phase, as with seasonal flu in which there may be localised outbreaks, mainly in specific institutionalised settings, is much more likely.
The problems with Michie’s thesis are underpinned by the false assumption that asymptomatic spread is a major driver of transmission. There is no robust evidence for this phenomenon, and it would go against decades of understanding of respiratory viruses and how they are transmitted. By continuing to disseminate this questionable hypothesis to the British public, she is continuing to spread unnecessary fear. A far more balanced approach would be to focus on:
1. The viral season rapidly waning
2. The huge percentages of vaccinated people & those with acquired or innate immunity
3. The fact that children are not a significant driver of the disease
4. The fact that clinical symptoms are the driver of transmission of respiratory viruses
We need to stop ‘acting like we’ve got it’ and start living what is left of our finite lives.
Data not dates
It was reported this week that the weekly COVID-19-related death toll has fallen to the lowest rate since October. However, in a scenario of ever-decreasing death rates and diminishing prevalence of the virus, a comparison to the COVID mortality rate at the beginning of the winter wave seems somewhat arbitrary and of no relevance to the current situation. Once deaths reach minimal levels, this indicates that cases must have been minimal 18 days earlier.
A far more sensible metric for comparison would be the current test positivity rate. Since 21 March the PCR positivity rate has been only 2.1% i.e. only 1% higher than the baseline positivity rate we saw in summer. Including all testing, only 0.43% of 1.2 million tests were positive on 29 March. To put this in perspective, 9,957 people tested negative out of every 10,000 tests done. Remaining locked down under these circumstances indicates that the Government has adopted a “Zero Covid” strategy, despite their own admission of the futility and harm that would be caused by attempting this policy. Patrick Vallance himself said: “I think the chance of eradication, true eradication – ie zero – are in themselves close to zero.”
Tracking the success of the vaccine and maintaining confidence
Last week, Sir Christopher Chope MP and William Wragg MP raised important questions in the House of Commons regarding COVID-19 deaths following coronavirus vaccination. Health Secretary Matt Hancock responded ‘I think we do have it’. Hancock also referred to the SIREN study but this only covers healthcare workers and therefore does not provide the complete information required for monitoring adverse effects, safety and efficacy. HART would urge active data capture, including a simple vaccine history taken at every unscheduled attendance at a hospital.
We must not forget that these are experimental vaccines, without full regulatory approval but issued under emergency waivers. It would be concerning in the extreme if data were not being collected or if the level of scrutiny of vaccine effects was not sufficient. The availability and rapid access to this data is vital in maintaining the public’s confidence in the vaccination programme.
US states continuing to open up
Governors across the US are continuing to open up their states and remove COVID-19 restrictions. Earlier this month, Mississippi and Texas both announced the end of business restrictions and mask mandates, while North Dakota went a step further and implemented legislation to make mask mandates illegal. In Florida, Governor DeSantis is to forbid vaccine passports with an executive order.
In Texas, COVID-19 cases and hospitalisations carry on their downward trajectory despite their removal of measures being described variously as: “absolutely reckless” by California Governor Gavin Newsom, “it just is inexplicable why you would want to pull back now” by Dr Fauci and “neanderthal thinking” by President Joe Biden.
Essential viewing
Nick Hudson, co-founder of the international group Pandemics ~ Data & Analytics (PANDA), has given a keynote address at the inaugural BizNews Investment Conference in South Africa. In his speech, Hudson gives a comprehensive overview of the COVID-19 pandemic and explores how instead of helping to slow the spread of the virus, lockdowns have led to infant mortality, poverty, starvation, joblessness and a major upsurge of psychological disorders. Well worth taking 30 minutes to watch in full, here. This video is currently being viewed by several thousand people per hour.
24 March 2021
There is no emergency
COVID-19 cases are low and all-cause deaths are now back to normal pre-pandemic rates and falling. All vulnerable groups have been offered a vaccination. There are no longer any justifiable or ethical reasons for prolonging Covid-related statutory ‘emergency powers’.
It is anticipated that all phase 1 priority groups (approximately 32 million people) will have been offered a vaccine by 15 April, a group accounting for 99% of the deaths last spring. This will be an amazing achievement. The virus is now endemic and will circulate at very low levels this summer and is then likely to join the range of respiratory viruses circulating each winter. Talk of continuing social distancing and masks for several years is therefore unnecessary and unhelpful. We urgently need to reduce fear and increase hope as we recover from this crisis.
It is vital that we harness the benefits of the rapid vaccine rollout by acknowledging we are no longer in an emergency. We can and must reopen society. Government and SAGE will need to undo the negative messaging, after a year in restrictions many people will still be fearful to pick up their lives again. News that a £2m Government contract has just been awarded for a COVID Public Information Campaign over the next two years is concerning. The repeal of the coronavirus emergency legislation would give a very positive message of confidence and hope to the British public. Therefore, HART continues to urge all MPs to vote against the renewal of the Coronavirus Act this week in Parliament.
No evidence of SARS-CoV-2 in schools
HART predicted 24,000 false positive results in children in the first week of mass testing based on 4 million children being tested twice. In the week of 4 March, only 2.7 million tests were carried out on secondary school children and 0.05% of them were positive. Our previous prediction was based on the estimated false positive rate for the adult population of 0.3%. Testing of university students prior to Christmas showed a very low false positive rate of at or below 0.06% including Newcastle, Hull, Exeter and Birmingham. Testing among school children is demonstrating a similar rate. The good news is that these numbers are so low that no-one can be left in any doubt that they represent only false positive results and that there is no SARS-CoV-2 at present in the secondary school population. The ONS estimated that there would be SARS-CoV-2 in 0.4% (1 in 250) 12-24 year olds, so this is another instance of failed testing with PCR. With no virus in schools, there is now no justification for the mask mandate or mass testing.
Is mask wearing benign?
This week, Dr Mary Ramsay from Public Health England told the BBC that face coverings were a ‘lower level restriction’ that ‘people can live with’ and they should continue to be worn ‘for a few years’. Her words are similar to those used by politicians to justify the introduction of the mask mandate in summer 2020, when it was portrayed as an extra layer of protection, a precautionary measure, a nothing-to-lose restriction.
While there is no evidence that masks significantly reduce transmission when worn routinely in real-world settings, there is recognition that they may constitute an infection hazard, particularly when used incorrectly. Masks potentially cause physical harms, while the social and psychological cost of concealing our faces from other people is considerable. Face coverings impair all forms of communication and human connection, make lip-reading impossible for the deaf and constitute a gross impediment to children’s social development.
A highly visible reminder that danger is supposedly all around, face coverings are fuelling widespread, irrational fear at a time when the current viral threat is very low and the vulnerable have been vaccinated. As we look to re-activate the economy and reopen our society, this mask-induced fear will act as a major obstacle. HART believes the Government should now lift the mandate and allow people to decide for themselves whether to wear one. It is time to trust the public with their own personal risk-based decision making.
The futility of border closures
Summer holidays are in doubt again, with the news that a £5,000 fine will come into force for anyone trying to travel abroad without a ‘reasonable excuse’. Matt Hancock has said the restrictions are to ‘guard against’ new variants that might put the vaccine rollout at risk. Professor Neil Ferguson was also quoted as saying we ‘should be planning on summer holidays in the UK not overseas’. Closing international borders to keep out ‘foreign mutants’ of an already endemic virus is neither useful nor possible. It is worth noting that mutant variants from abroad pose no extra threat compared with any homegrown variants and are likely to have very similar sequences. Mutant variants, emerging overseas or domestically, are an inevitable biological reality once a virus is in the population, as is the case in the UK. The virus will mutate slowly over time, irrespective of borders.
Mandatory vaccination for care home workers
The news that the government is considering making COVID-19 vaccination a legal requirement for all care workers is concerning and against international law. This would create a precedent of eroding informed consent, and is difficult to justify when the vulnerable population have themselves already been offered at least one dose of vaccine, especially in the light of Scottish data that suggests the Oxford-AstraZeneca vaccine reduces risk of hospitalisation by up to 94%. If this is case, would it be better to prioritise second doses for all vulnerable groups, thus rendering the vaccination of our younger, healthy population unnecessary?
And some good news…
The number of patients admitted per day to intensive care units is now close to normal, pre-pandemic levels for the time of year. It appears we are well beyond the risk of overwhelming the NHS – further highlighting that now is the time to lift restrictions and allow the NHS to begin rapidly addressing the backlog of postponed appointments and operations. There is no sign of a virus resurgence in American states such as Florida and Texas which have lifted restrictions.
Related
Will the proven Covid-fighting drug Hydroxychloroquine now be allowed to save lives?


